Note: “An Arm and a Leg” uses speech-recognition software to generate transcripts, which may contain errors. Please use the transcript as a tool but check the corresponding audio before quoting the podcast.
Dan: Hey there! A couple of months ago, we asked you to help us report on a type of fee that seems to be sneaking onto more and more medical bills. They’re often called “facility fees.” It’s like a cover charge just for walking in the door. And these kinds of fees are familiar to a lot of folks from places like emergency rooms, which do have a LOT of specialized equipment and staff in the facility behind that door. That’s basically the case for a cover charge: Once you get in the door, there’s a lot of stuff there. But in some cases, with facility fees, the door is just the entrance to a doctor’s office. Because facility fees– they’re often charged by hospitals. And hospitals own a lot of doctors’ offices these days. And once they take over, there’s no law that says they can’t just call that doctor’s office part of their facility and start charging.
We asked what you’d been seeing. A bunch of you sent us stories, and copies of your bills, and your insurance statements. And when we called to follow up, you took our calls. You had A LOT to say.
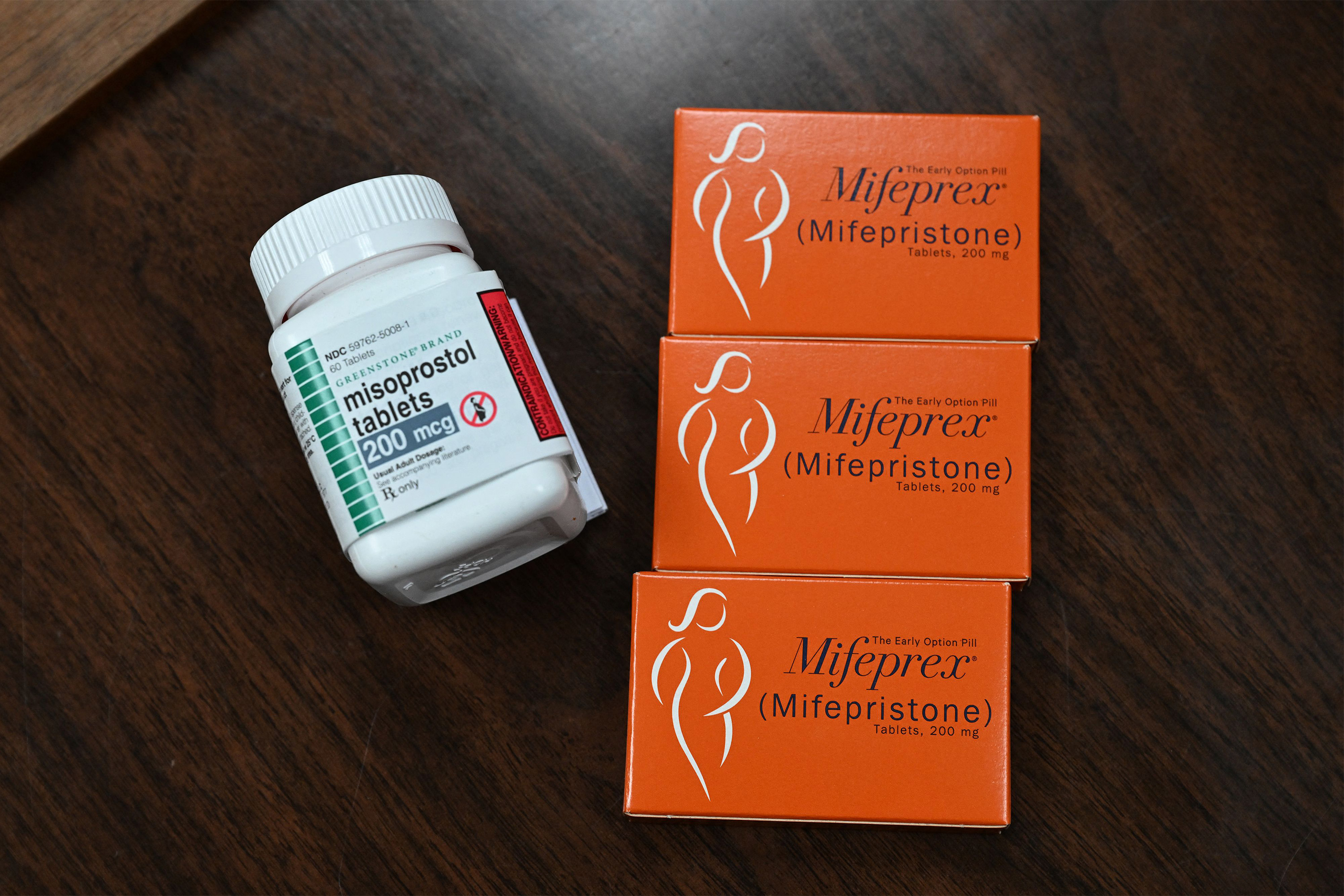
Teresa: Oh, it made me so mad, so mad. Anne: I mean, it’s a 10-minute appointment for a prescription.
Amanda: I don’t understand any of it. Where did this number come from?
Dan: We learned a bunch. Especially from those of you who are not new to this kind of thing.
Francesca: It was a running joke with my husband and myself that like, okay, it’s time for my weekly, one-to-two hour phone call with Cigna.
Dan: People who’ve been contending with the health care system for a while, dealing with chronic illnesses, or going to the doctor for monitoring, or having some kind of ongoing treatment.
Anne: I see her once a year. I’ve seen her once a year for 18 years at the time. And then they started charging the facility fee.
Dan: And I’ve always said here, we have a lot to learn from each other. And what we learned here is a lot more than is gonna fit in one episode. So we’re gonna start here with one story that really stood out. Partly because it involved the biggest dollar amount we saw: An eight-thousand dollar facility fee. And partly because the person we heard from … didn’t end up paying it. And partly because of what it took for her to avoid paying it. She had what I might call a lifetime of preparation– including lessons I think a lot of us can learn from. And she has the kind of grit that not all of us have. But I’m hoping that some of it might rub off. So let’s meet her.
Georgann Boatright: My name is Georgann Boatright, and I am a retired speech pathologist.
Dan: Georgann lives in Oxford, Mississippi. She works for the university there, Ole Miss, coordinating special events.
Georgann Boatright: It’s lots of fun. Never a dull moment. Everything from weddings to conferences.
Dan: The day we talked, she had made coffee for 500 people. Before eight am. And here’s how she describes her response to that eight-thousand dollar charge.
Georgann Boatright: I was like, that’s insane. And of course, being the obnoxious human being that I can be at times, and a little bit pushy, you know; sometimes you got to do that. I’ve always been that advocate for everybody else, so sometimes I have to advocate for me.
Dan: Georgann pushed back– we will talk about how far she had to go. And among other things, we’re talking about actual miles she had to travel. It was not easy. But it was worth it. Let’s take a ride.
This is An Arm and a Leg– a show about why health care costs so freaking much, and what we can maybe do about it. I’m Dan Weissmann. I’m a reporter, and I like a challenge. So the job we’ve chosen here is to take one of the most enraging, terrifying, depressing parts of American life, and bring you a show that’s entertaining, empowering, and useful.
Georgann Boatright grew up in Oxford, went to Ole Miss– the University of Mississippi, right in town. And after a decade and change in places like Huntsville, Arkansas, and towns near Springfield, Missouri, she moved back to Oxford about 15 years ago.
Georgann Boatright: My mom came ill. And so I moved back to Mississippi to be with her for the end.
Dan: Georgann herself had a health scare not long after– it turned out to be a non-cancerous tumor. Her local doctors couldn’t figure out the problem, but she found good treatment at West Cancer Center in Memphis, about an hour and a half away. And then, in 2022, an actual breast cancer diagnosis. She went back to the West Cancer Center in Memphis for treatment. And while she was being treated for breast cancer, her doctors found a thyroid problem.
Georgann Boatright: But they were kind of like, okay, we’ll put that on a back burner for right now because we got to take care of this first.
Dan: So, they did! And you know, that took months, of course. Once she was done– and no evidence of cancer for a few months!– they picked up the thyroid thread. Her endocrinologist in town suggested what’s called a needle biopsy: no incision, just pulling a sample with basically a syringe, guided by ultrasound. And Georgann was plenty familiar with the procedure because she’d had two of them for her breast cancer.
Georgann Boatright: Well, of course, having just done all this other stuff, I was kind of like, oh, okay, just another biopsy. No big deal.
Dan: Her endocrinologist suggested the local hospital, Baptist Memorial, North Mississippi. And started getting her scheduled there.
Georgann Boatright: I was just sitting in my office doing my thing and, you know, answering emails, trying to get people to sign up and do a wedding. So, they called me and said, “Hey, you know, we need a thousand dollars up front.” And I’m like, why? I’ve already met my deductible. Da, da, da. You know, and they’re like, Oh, well, this is just this is just your copay.”
Dan: None of this sounded right to Georgann, based on her experience.
Georgann Boatright: I’d had two biopsies done in the past year, just in the process of doing the breast stuff. And I was like, that’s not normal.
Dan: At the cancer center in Memphis, a thousand dollars was in the ballpark for the whole procedure, like before insurance paid anything. And Georgann’s share, after insurance, was like a fraction of that.
Georgann Boatright: And I went, excuse me, because of course I was expecting, you know, under a hundred bucks, you know. And they acted very offended that I questioned. She was like, “Well, this is standard.” And I was like, “But I’m confused,” and, you know, and the more questions, she got kind of defensive.
Dan: Georgann says she quickly developed a little sympathy for the woman on the other side of the call.
Georgann Boatright: I was like, this person has no clue. This is their job. They’re given this information. They’re given my phone number. They’re told to collect a thousand dollars from me. You know, I mean, it’s not her fault.
Dan: So, Georgann quickly made a new plan. First step: get a line-item version of that estimate, in writing. And next: find somebody else to talk with.
Georgann Boatright: I was like, “Well, hey, how about you just do me a printout and I’ll come by the hospital and pick that up. If you’ll just leave it with somebody near the desk …”
Dan: … Then Georgann figured she can actually see what these charges are for and you know, maybe talk to somebody who’ll know a little more. She went that same day.
Georgann Boatright: I wanted to get the biopsy done. I wanted to find out what was going on. You know, once you’ve had cancer, it kind of, that C word just does not sit well with your brain. You kind of, it starts eating at you and you’re like, I really want to know.
Dan: And she wanted to know why the hospital wanted a thousand dollars from her. She got that printout– the line item estimate. It showed thirteen thousand dollars in charges. And the single biggest charge– more than half of the whole bill– eight thousand dollars– was for an “operating room” charge. It wasn’t labeled “facility fee,” but that’s exactly what it was. Georgann sent us this line-item estimate. We showed it to a medical-bill coding expert; she confirmed– this is a facility fee. And I’ll just mention again: Of all the people who sent us bills with facility fees on them, this was the highest by a LOT. Alot a lot. And seeing this “operating room” charge really set off alarm bells for Georgann. Because Georgann had just had TWO needle biopsies. And they sure as heck had not taken place in an operating room.
Georgann Boatright: It’s a needle aspiration. It is ultrasound-guided. So it’s done in radiology. This is not in an operating room.
Dan: When she got to Baptist, Georgann did get to talk in person with a billing specialist. It wasn’t a satisfying heart-to-heart, but it gave Georgann the clarity she needed.
Georgann Boatright: At a certain point in the conversation, I was just kind of like, “You do realize that there is not an operating room involved in this?” And she said, “Well, of course, there is.” I was like, “No, there really isn’t.” “Oh, well, that’s just our standard procedure.” And so she stuck with that. And so I was like, okay, well, since you’re going to just stick with this, I’m going to just let this go. Because if I can’t seem to get you to understand that I’m not going to pay you 8,000 dollars for an operating room that I’m not going to go in, we’re not going to get anywhere.
Dan: And Georgann knew she had an alternative: She could go back to the cancer center in Memphis. It was a bit of a drive, but she trusted them to do good work and not to overbill her. So that’s what she did. Her out of pocket cost was eighty dollars. We asked Baptist all about Georgann’s experience, and what was behind this eight-thousand dollar charge. Especially since medical and surgical supplies were listed as separate line items.
A hospital spokesperson wrote back: “The price a patient sees on the hospital bill also reflects all the people who care for them and keep the hospital operating, not just the services provided, such as nurses and caregivers at the bedside, pharmacists, lab technicians, food service staff, environmental service professionals and security personnel who, among many others, keep the hospital running 24/7. We believe we charge fair and reasonable prices for our expert care.”
Of course, we also asked Baptist why there would be an operating room charge at all, when the patient didn’t expect to be seen in an operating room. The spokesperson wrote back: “I’m not sure why there was a discrepancy. But, in general, the pricing information we share with patients is only an estimate, and the final bill can vary. We encourage patients to contact us with any questions.” OK, then. And I just want to say: I think– well, I KNOW– that I’ve undersold what it took for Georgann to make that decision. I mean, yeah, we’ve seen, Georgann showed a lot of initiative, and savvy, and decisiveness, and a certain amount of grace in navigating a couple of conversations with her local hospital’s billing department. But we haven’t seen EXACTLY what made her so prepared for those conversations, and to make her decision so quickly. And if we’re gonna learn from Georgann’s example, we’ve gotta look at that. That’s coming right up.
This episode of An Arm and a Leg is a co-production of Public Road Productions and KFF Health News. Public Road is the organization I founded to make this show. The name comes from Walt Whitman; I’ll tell you about it sometime. KFF Health News is a nonprofit newsroom covering healthcare in America. Their journalists do amazing work– win all kinds of awards, every year. I’m honored to work with them. So, what allowed Georgann Boatright to navigate those conversations with her hospital billing department so skillfully? And to quickly decide to drive to another city for care? Well, let’s start with her old job as a speech pathologist. You might remember, when she did that job, she was living in places like Huntsville, Arkansas. Or, as Georgann describes it …
Georgann Boatright: … Absolutely the middle of nowhere, Arkansas.
Dan: It’s not like a speech therapist is gonna have a ton of clients in town. Georgann worked for an agency that sent her all over the place.
Georgann Boatright: I was driving about three- to five-hundred miles a day when I retired.
Dan: A day!
Georgann Boatright: Yeah, well, they’re spread a little thin in that area.
Dan: Yeah. Yeah. Right. How fast were you driving? Like, how many hours are we talking about being on the road?
Georgann Boatright: I was usually on the road 12 to 14 hours a day.
Dan: Oh my god.
Georgann Boatright: Yeah, but that’s because, you know, I was bouncing in and out everywhere from Liberty, Missouri, which is outside of Kansas City, all the way down into Arkansas.
Dan: So, we start to get the idea that driving an hour and a half from Oxford to Memphis is, you know, not such a big deal to Georgann. But there’s this other thing. Which is what Georgann spent all those hours in her car actually doing. Because she was not listening to podcasts, I can tell you that. She was dealing with health insurance. On behalf of her colleagues and her patients.
Georgann Boatright: I was the person in our company that would do all the appeals. I got really good at getting Medicare, Medicaid, Blue Cross Blue Shield– all the insurances to pay.
Dan: Georgann did all this by phone, with somebody back at the home office transcribing for her. It was part of her gig– because she had all that time in the car. The agency she worked with also employed physical therapists and occupational therapists, sending them out to nursing homes. And those colleagues would have multiple appointments a day at the same spot.
Georgann Boatright: I would only have like, maybe one or two patients during the course of the day, and then I would end up doing paperwork the rest of the day or helping someone else do paperwork.
Dan: Because not only did Georgann have time with all those hours in the car. She had something else: language skills.
Georgann Boatright: The crew that I worked with, they were mostly from the Philippines, and we partied very well. And I ate a lot of good food, and I gained weight. And no fault of their own, English wasn’t their first language. So that was part of my job was to make sure that the language barrier wasn’t the problem for the physical and occupational therapists getting paid.
Dan: So for five years, she spent most of her long workday dealing with insurance.
Georgann Boatright: That was what I did, and I was really, really good at it. You know, when you get on a first name basis with the reps in your area, you know that you’re a thorn in their side. When they would see my name, they’d be like, “We might as well just go ahead and pay this one because she’s going to find a way to get it through.”
Dan: So when Georgann ended up talking with those folks at her local hospital’s billing office– the folks who were trying to tell her that an eight-thousand-dollar operating-room fee was just standard– she had a pretty good idea of what their jobs were: Just getting the hospital’s money.
Georgann Boatright: I get that. And I understand that, but you know, you have to understand when you’re calling people and asking them for money that you have to know why they’re paying you money and whether or not you can justify how much they’re paying you.
Dan: So, just to recap: When Georgann was in those conversations with the local hospital billing department, she had years and years of experience in medical billing. She was, by her account, really really good at it. It doesn’t seem like a stretch to guess that when she talked with these folks at the local hospital’s billing department, she knew a lot more about medical billing than they did. And she knew that this hospital wasn’t her only option. She had just done cancer treatment at West Cancer Center in Memphis. She trusted them, and they hadn’t overbilled her. And she wasn’t afraid of a road trip. That 300-mile, 500-mile-a-day job was a while ago, but just in the last year she’d made the trek to Memphis for cancer treatments, several times. In fact, the story of the wrap-up to that treatment gave me real appreciation for Georgann Boatright’s brand of cheerful grit and determination. For more than a year, Georgann had been planning a big family reunion for Christmas: Her kids, their kids, gathered from across the country, to a lodge near her husband’s mom.
Georgann Boatright: I wanted his mom who has been getting on in age to get a chance to see the great grands and this kind of stuff.
Dan: Georgann had made the reservation for the lodge months before her cancer diagnosis. And then, the last day of her radiation treatment got scheduled for December 23. The reunion was scheduled to start that very night. In Branson, Missouri– a five-hour drive from Memphis.
Georgann Boatright: And I was like, I am not canceling this. Everybody’s like, “Mom, you don’t have to do this,” blah, blah, blah. I was like, “No, I’m going to be healthy and done with this treatment. By the time of this reservation.” I said, “I don’t care what happens!”
Dan: The procedure that last day was to remove a device that had been delivering targeted radiation doses. And when the day came, an ice storm knocked out the power at West Cancer Center. The medical staff suggested, you know, rescheduling.
Georgann Boatright: They’re like, “Well, do you want to come … No! I want this done. I am not coming back tomorrow.
Dan: Wow.
Georgann Boatright: I am going to make this reservation. I’m going to spend the night in a very nice place in Branson, Missouri and play in the snow.
Dan: It wasn’t gonna be easy.
Georgann Boatright: There was no power. There was no lights. There was only the little emergency generator lights that come on in a hospital.
Dan: But they made it work.
Georgann Boatright: I had it taken out that day. By the flashlights of the nurses
Dan: The flashlights on the nurses phones! Georgann says she slept in the car while her husband drove them to Branson that day. Mission accomplished.
Georgann Boatright: It was a great trip, and everybody was there, and it was wonderful to kind of celebrate at the end of that. I was done with radiation. I was like, I’m going to get well now and just keep kicking cancer’s butt. Because I was like, I am not giving up.
Dan: I said right at the top: This story is epic, right? And I said that whatever’s powering Georgann Boatright, I hope just a little bit of it can rub off on us– on me. So, when Georgann talked with the folks in the billing department at her local hospital, she knew just what she was capable of. Also, it’s worth mentioning, she knew she had some other things that not everybody has: She knew she had excellent insurance because she’d seen it at work when she got the bills for her breast cancer treatment. And she knew she had someone to drive her to Memphis and back. Uber? That would’ve cost a LOT. Actually, Georgann says she priced it recently for her job.
Georgann Boatright: It’s 145 dollars, and I was like, you got to be kidding me!
Dan: I believe I could fly to Memphis from Chicago for 145 dollars one way.
Georgann Boatright: I could get a flight to Southwest for 120. Believe me, I do it. That’s my thing. If I do it during the week, I can go from here to Midway. Yeah.
Dan: Wait, why is flying to Chicago’s Midway airport Georgann’s thing? Well, the answer actually relates to one more thing Georgann had going for her in this whole scenario. Something– someone– I left out before.
Melissa McChesney: My name is Melissa McShesney. I live in Chicago, Illinois.
Dan: Melissa is Georgann’s daughter. She is the mom of two of Georgann’s grandkids. Melissa’s brother– dad to three more grandkids– he also lives in Chicago. Those kids and grandkids are, all of them, the reason Georgann has that airfare at the tip of her tongue. But it’s Melissa who plays a role in this story. Because Melissa works for CMS, the Centers for Medicare and Medicaid Services– the federal agency that oversees Medicaid and Medicare. So health insurance is her job. I mean, at least government-funded insurance.
Melissa McChesney: I only know enough to be dangerous on the private side. But, you know, I have colleagues that know a lot more.
Dan: Melissa and her mom– two health-insurance experts– can back each other up.
Melissa McChesney: It’s always great to have another set of eyes. So, sometimes I call her, sometimes she calls me.
Dan: This time– after those conversations with the hospital billing department– it was Georgann who did the dialing.
Melissa McChesney: She called me to say, “This doesn’t make any sense. Why is this the most expensive procedure I’ve seen in a year when I just went through breast cancer treatment? At least from the out-of-pocket cost. And I quite frankly didn’t fully know either.
Dan: So some poking around led Melissa to a story from the Bill of the Month series our pals at KFF Health News do with NPR.
NPRHost: For our September bill of the month, we’re taking a close look at facility charges …
Dan: And this story was a pretty exact match with Georgann’s situation: An operating room charge for a needle biopsy. NPR’s website even had a PDF of the original bill, with the billing codes.
Melissa McChesney: Which was very helpful, actually, because I was able to see the fee that the article was focused on. And I was like, “This is the exact same thing, mom.”
Dan: And that bit of context? It confirmed for Georgann that she could trust her initial impression: That this “operating room” fee seemed out of whack. And that she could do better. So she had that biopsy at West Cancer Center in Memphis before the week was out. And good news: She’s OK! The biopsy came back benign. Her local endocrinologist has been monitoring her bloodwork.
Georgann Boatright: And so right at the moment, my thyroid levels are all staying normal. So they’re not concerned that it’s throwing off everything unless it becomes like a huge thing that grows in my neck.
Dan: And she gets an occasional ultrasound at a local clinic. No needle, no hospital, no facility fees– and keeping an eye on the bills.
Georgann Boatright: They have been very reasonable. That’s why I was like, okay, well I’ll continue doing this as long as y’all don’t screw me over anymore.
Dan: One last thing I should tell you about Georgann and how she handled that eight thousand dollar charge the hospital had wanted: This is something she did after her daughter Melissa sent her that NPR story– you know, the one that helped her decide she was definitely going to Memphis. Melissa’s got this part of the story.
Melissa McChesney: She sent the NPR article and her estimate to her endocrinologist and said, “Just so you know, this is what happens when you refer individuals to this hospital. And you know, it would cost them a lot of money.” I was so proud of her for doing that. it just speaks to my mom and trying to be a person who’s not just worried about her own experience, but the experience of others in her community.
Dan: I’m telling you, we all want some of Georgann Boatright to rub off on us.An ArmandaLeg Season 12, Episode 1 July, 11, 2024 p.14 You sent us SO MANYstories about facility fees. I hope you can see why we wanted to bring you this one first, but we are not done. We talked with a bunch of you– and we talked with some experts who gave us some insights … and some lessons.
Shelley Safian: Sometimes you talk to the physician, sometimes you talk to the facility, sometimes you got to go to the president and say, “You know what? This is not right.”
Dan: And we talked to experts who gave us a look at what policy makers all over the country are doing– or trying to do– about these fees. Because they’re definitely paying attention. Because a lot of people are recognizing: You should not need to be Georgann Boatright to find a way around fees like this. Most of us aren’t.
Christine Monahan: There’s bipartisan interest in this issue. We are seeing these reforms bubble up across the states.
Dan: So over the next couple of months, we’ll be sharing a LOT more of what you’ve been helping us learn. Meanwhile, because you’ve been so incredibly helpful here, I’m going to come back to you soon asking for more help on a different story. That’s coming next time. Till then, take care of yourself.
This episode of An Arm and a Leg was produced by Emily Pisacreta and Claire Davenport, with help from me, Dan Weissmann, and edited by Ellen Weiss. Adam Raymonda is our audio wizard. Our music is by Dave Weiner and Blue Dot Sessions. Gabrielle Healy is our managing editor for audience. Gabe Bullard is our engagement editor. Bea Bosco is our consulting director of operations. Sarah Ballama is our operations manager.
An Arm and a Leg is produced in partnership with KFF Health News. That’s a national newsroom producing in-depth journalism about healthcare in America and a core program at KFF, an independent source of health policy research, polling, and journalism. Zach Dyer is senior audio producer at KFF Health News. He’s editorial liaison to this show.
And thanks to the Institute for Nonprofit News for serving as our fiscal sponsor. They allow us to accept tax-exempt donations. You can learn more about INN at INN.org.
Finally, thank you to everybody who supports this show financially. You can join in any time at https://armandalegshow.com/support/. Thanks so much for pitching in if you can– and, thanks for listening.